
My life change this morning. For the good. And, for regular readers-no, it’s nothing related to my current cancer treatment.
It’s the day after Hawaii’s Primary Election, and normally that involves my spending hours knee-deep in raw text files and legacy database queries.
But today was different. And that’s how the story begins.
In the past, my first task in the morning after an election, even before getting a cup of fresh coffee, would be to visit the Office of Elections’ website and quickly eyeball the tables of election data from the most recently available statewide summary of results. After a quick look through the outcomes of what were expected to be the most contested races, I would then download the text file containing raw precinct-level data also available from Office of Elections.
The next task would be to import the text file into Filemaker, a robust Mac database. My version is about five years old, but perfectly serviceable for my uses.
Once the data was downloaded into Filemaker, I could then begin converting my questions into queries instructing Filemaker how to search through and analyze the data from different directions, breaking it down to precincts or summarizing by electoral districts or neighborhoods looking for patterns. Sometimes I started with specific questions, but lots of times I just wanted to satisfy my curiosity. Occasionally I might share some findings in a post-election blog post, but more often they just provided background understanding to guide my future reporting. And many times I would be stalled out trying to write a query that produced exactly the results I was looking for.
Then the earth moved!
This morning, I skipped the whole text file/download/import/Filemaker process and decided to see how far I could get by simply letting an AI assistant do the heavy lifting.
After downloading the plain-vanilla statewide table of precinct-by-precinct results in pdf format from the elections website, I just uploaded the 498-page data table to Claude, Anthropic’s AI assistant and the dog I chose for today’s hunt.
Claude was immediately ready to rock and roll!
I had been surprised to see how handily Congressman Ed Case had fended off what appeared to be a strong challenge from State Senator Jarrett Keohokalole, and wanted to know more about voting in their head-to-head race.
Working with Claude was seamless. I started asking questions, and Claude began returning clear, detailed answers instantly.
How many districts within Congressional District 1 did Keohokalole carry?
Claude’s answer–None.
Case ran the table, winning every one of the 25 legislative districts that make up the Congressional District 1. Claude did not include the two districts that are split between CD1 and CD2 because they didn’t fit my initial question.
And Claude provided an unexpected takeaway. The areas where Case showed the greatest strength are not where most observers might assume they would be.
Key takeaway: This is a stark geographic story.
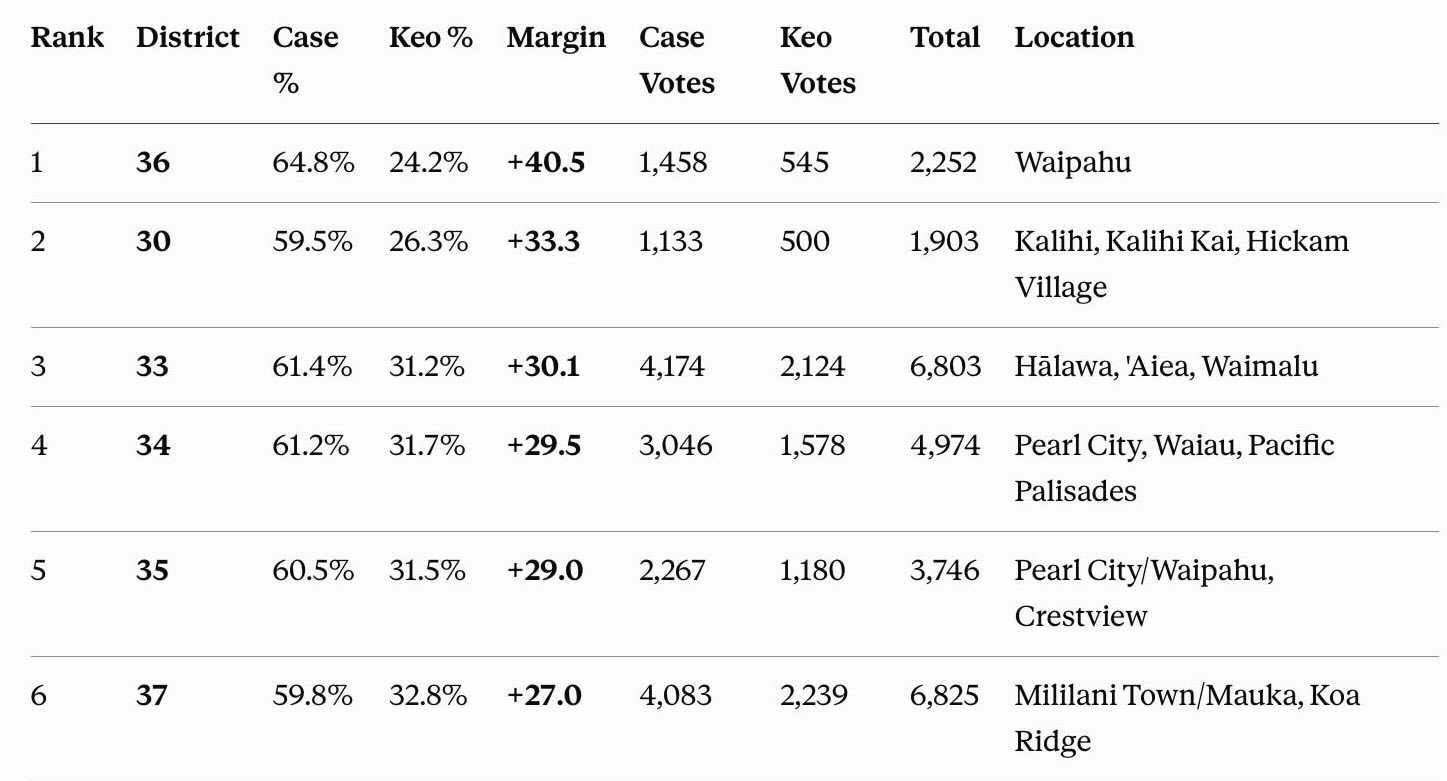
Case’s biggest margins over Keohokalole are almost entirely in Leeward and Central Oahu — Waipahu (District 36) crushed it at +40.5 points, followed by Kalihi, ‘Aiea/Halawa, Pearl City, and the Mililani corridor. These are working-class and suburban communities, not Case’s presumed home-turf advantage neighborhoods.
Notably, East Honolulu districts (18, 19, 20) — where you’d expect an incumbent’s strongest home support — only rank #9–12 on this list, with more modest margins (+16 to +20 points) despite being generally considered “Case country.” His dominance was actually strongest in the areas furthest from town.
Only 2 districts (21 and 46, not shown in top 25) had narrower margins below +8 — Case won every single House district in the congressional district, just by varying amounts.
In 1976, I doubt this geographic pattern would have been any surprise, as the leeward area at that time was considered the stronghold of the AJA-generation of Democratic Party organizers credited with the behind-the-scenes grassroots work that powered the party’s rise to political dominance. But the public perception is quite different today, making these findings somewhat startling.
Here are the districts where Case outpaced Keohokalole by the largest percentage margins. The full list can be found here.
I chose Claude for this assignment more or less at random, and I expect other AI assistants would provide more or less similar answers. That’s probably a hypothesis worth testing another day. What I keep coming back to, though, is Waipahu and Leeward Oahu. The strongest support for this four-term congressman considered to be at the more conservative end of Hawaii’s Democratic Party spectrum strongest ground wasn’t in the politically purple districts in East Honolulu — it was in the traditional Democratic Party strongholds from Pearl City to Waipahu. The progressive drift of many Democratic activists appears to carry less sway out thata way.
Twenty minutes with a PDF and an AI assistant got me to that insight almost before I’d finished my coffee. A few years ago, that would have taken me the better part of a morning, if I got there at all.


